Note: this a really basic discussion of a very complex and ever-evolving topic.
The genetic information that codes for traits in all living organisms are found in DNA or RNA or a combination of the two. Even viruses, not really seen as living organisms, have genetic material. They either code them in RNA (RNA viruses) eg. Influenza or DNA (DNA viruses) eg. Herpes.
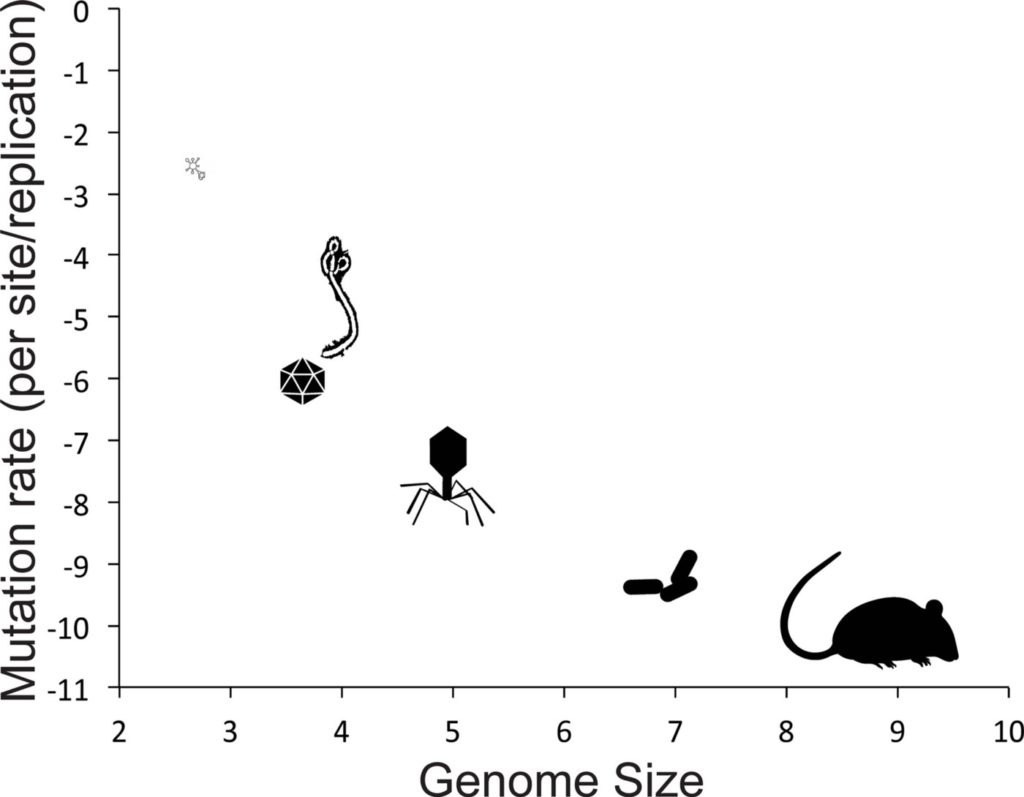
Where DNA viruses are quite big, RNA ones are much smaller. Also, RNA viruses replicate (multiply) way more than DNA viruses.
(Just a reminder, DNA and RNA are made up of bases called nucleotides).
To exert their disease-making effects all viruses have to enter the cells of the organism they are attacking. So they find a receptor that fits them on the membrane of the cell, fuse with that receptor and then worm their way into the cell.
Once in the cell, a DNA virus finds its way into the nucleus of the cell and fuses with the host organism’s DNA. As it divides and multiples, it uses the organism’s enzymes it needs for multiplication — the polymerases. Ensconced in the nucleus, DNA viruses tend to be more stable over time. They multiply and mutate less and therefore may be easier to treat.
The RNA virus on the other hand, stays in the cytoplasm and divides in there, using its own polymerases. Being smaller, using its own polymerase and away from the influence of the host organism, the RNA divides very fast and often. This leads to the RNA virus being able to switch out the nucleotides in its RNA often resulting in a different strain than what entered the organism — a process we commonly term “Mutation”!
It has been calculated that RNA viruses mutate on an average of once every 50,000 base pairs per infection. DNA viruses do that once every 50,000,000 base pairs per infection.
Now DNA viruses have mutations too but one, they are not as frequent and besides, the organisms polymerases can cut out these renegade nucleotides. The RNA’s polymerases lack this repair ability.
Mutations in RNA viruses are often set off when the environment in the cell changes — like when it senses the presence of a new vaccine or antibodies or medications. This ability to multiply fast and often is the reason why we never seem to get a good enough vaccine for the flu. That is why we sometimes need to treat viral infections like HIV and Hepatitis C with more that one medication.
This ability to mutate often also leads to instability of the RNA virus — it can generate a lot of mutants which do not survive or which may even be more virulent. Much more virulent than the organism that entered the cell.
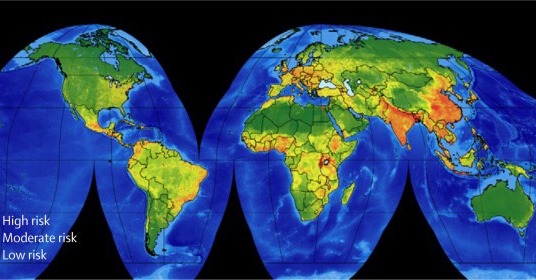
Now in most normal humans, the body is able to mount a level of immunologic reaction to the vast number of viruses that affect humans. However, if the virus is totally new to humans, that ability is not available for months to even a year. Thus when a novel RNA virus spills over from another mammal into a human, those initial months to a year are very unpredictable. We are dealing with a virus that can mutate into a more virulent strain and against which the body still has no defense.
COVID-19 is an RNA virus that spilled over recently!